PROMO!
First order? Get 10% OFF with this code: 1storder
Written by

Diabetes affects millions of people around the world and leads to serious health problems. Research shows that the ARA-290 peptide may help ease some of these problems.
It targets special receptors in damaged tissues. Studies suggest it may reduce neuropathic symptoms and improve nerve health in people with diabetic nerve damage. In recent years, ARA-290 peptide research has helped us better understand how to treat diabetes-related issues.
At the same time, studies are closely checking for any safety issues as research moves forward. These peptides are made only for research use and are not for human use.
Animal studies using knockout mice have helped researchers learn how this peptide works. In clinical trials, there was statistical significance when comparing nerve function between the treatment groups and the control groups.
To understand how ARA-290 peptide works, it helps to first look at the condition it is studied to target.
Explore ARA-290 Peptide from Peptide Works, a synthetic peptide researched for easing neuropathic symptoms and supporting nerve regeneration.

Diabetic neuropathy is nerve damage caused by diabetes. High blood sugar damages the small blood vessels that supply nerves, reducing oxygen and nutrient delivery to nerve tissue.
Over time, this leads to numbness, tingling, and burning sensations. The three main types are peripheral, autonomic, and focal neuropathy. Peripheral neuropathy is the most common and typically affects the hands and feet first.
Poor control of blood sugar makes this condition more likely. Up to 50% of people with diabetes will develop some form of neuropathy.
Research into MOTS-c shows it may enhance insulin sensitivity and improve glucose metabolism in diabetic patients.
Among the types of neuropathy, learning why peripheral neuropathy follows a certain pattern helps us understand why it can be so serious.
Explore MOTS-c from Peptide Works, a mitochondrial peptide researched for improving glucose metabolism, insulin sensitivity, and heart protection in diabetes models.
Peripheral neuropathy affects the longest nerves first because they need more energy. These nerves, found in the feet and hands, get less blood flow than shorter nerves. High blood sugar causes nerve damage by harming the tiny blood vessels that feed these distant nerve endings.
Symptoms start as numbness, tingling, and burning in the toes. ARA-290 peptide research shows promise for treating small nerve fiber loss in these areas.
Studies suggest that up to 50% of diabetic patients may develop peripheral neuropathic pain. Research into MOTS-c peptide also indicates potential metabolic benefits, including prevention of obesity and hyperinsulinemia in high-fat diet models.
When these distant nerve fibers become damaged, the effects can extend beyond numbness in the hands and feet, affecting balance, sensation, and overall nerve function.

When small nerve fibers are lost, sensory and autonomic functions begin to decline. Small fiber neuropathy affects pain and temperature sensation, leading to burning pain, stabbing sensations, and reduced ability to detect temperature changes.
Damage to these fibers also disrupts autonomic control. Research shows small fiber neuropathy can affect sweating, heart rate, blood pressure, and digestive function, causing widespread symptoms beyond the hands and feet.
Inflammation also plays a role. Cytokine-driven immune responses contribute to nerve damage progression and worsening neuropathic pain in diabetic neuropathy.
Studies on ARA-290 show reduced neuropathic symptoms and increased small nerve fiber density, suggesting potential nerve repair and anti-inflammatory effects in small fiber neuropathy.
MOTS-c shows improved glucose regulation and prevention of high-fat-diet-induced obesity and hyperinsulinemia in metabolic disease models.
Loss of autonomic nerve fibers can become dangerous when cardiovascular control is affected, as cardiac autonomic neuropathy increases the risk of serious complications and mortality.
Small fiber damage disrupts the central nervous system control over cardiovascular functions. Damaged autonomic nerves cannot regulate heart rate properly. This causes resting tachycardia. Orthostatic hypotension develops when patients stand up quickly from sitting positions.
The sympathetic and parasympathetic balance becomes severely disturbed in these cases. Published clinical studies of metabolic control show improvements. These may help prevent adverse events.
Derivatives of recombinant human erythropoietin, like ARA-290 peptide, target innate repair receptor pathways. Researchers order from Peptide Works because we sell high-quality peptides with worldwide shipping.
These cardiovascular changes create immediate symptoms. Patients notice them during daily activities, especially when changing positions.

Dizziness when standing in diabetes is usually caused by orthostatic hypotension. This occurs when blood pressure drops by at least 20 mmHg systolic or 10 mmHg diastolic after standing, reducing blood flow to the brain.
Meta-analysis research shows orthostatic hypotension affects about 24% of diabetic patients, making it a common sign of autonomic nerve damage.
In diabetic autonomic neuropathy, damaged nerves cannot tighten blood vessels quickly enough when standing. Blood pools in the legs, lowering blood pressure and causing dizziness, lightheadedness, and visual dimming.
Visual symptoms occur because reduced blood flow temporarily affects the brain and eyes, showing that autonomic dysfunction impacts multiple organ systems simultaneously.
Vision may go dark when standing due to orthostatic hypotension, where blood pressure drops suddenly and reduces blood flow to the brain and eyes. This temporary reduction in cerebral and retinal perfusion can cause blurred or darkened vision lasting a few seconds.
Diabetic autonomic neuropathy increases this risk because damaged autonomic nerves cannot constrict blood vessels quickly when standing. This leads to reduced oxygen delivery to visual pathways and temporary visual dimming.
Research also shows that unstable blood pressure during standing can affect retinal and visual function, indicating broader vascular involvement in diabetic autonomic dysfunction.
Studies on ARA-290 peptide suggest activation of tissue-protective pathways that reduce inflammation and improve neuropathic function, which may support vascular and autonomic health in diabetic neuropathy research.
These temporary vision changes often signal broader autonomic and vascular dysfunction that may require further evaluation.
Eye doctors measure corneal nerve fiber density using special microscopes. This helps find early damage. The test shows nerve loss before symptoms of small fiber neuropathy in vision appear.
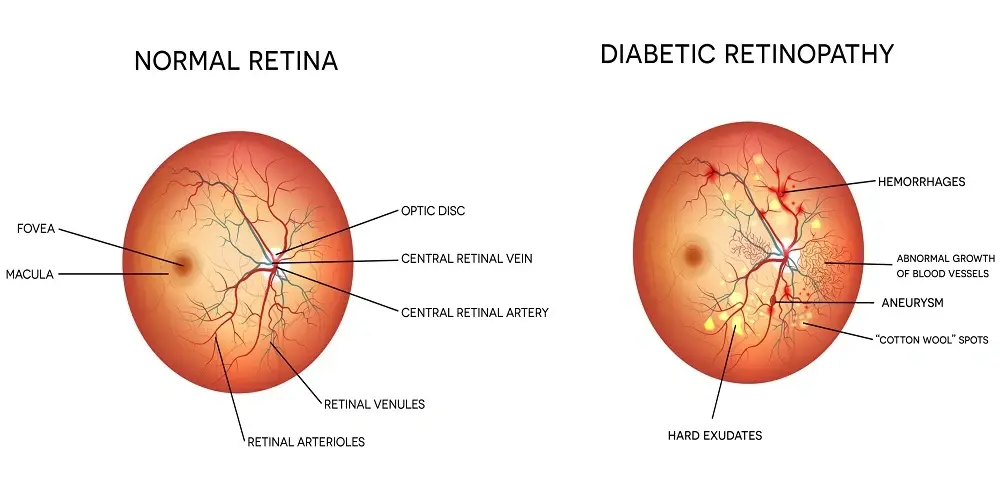
Diabetes mellitus causes significant changes in retinal photographs. Trained specialists can easily see these changes.
Patients often have night blindness, glare sensitivity, and trouble focusing on close objects. Clinical trial data shows these vision changes often happen before major complications. This highlights the importance of early detection.
ARA-290 peptide research studies how to protect corneal nerve fibers in lab models. Eye exams that find problems early help prevent bad outcomes in diabetic patients.
Night vision problems are among the first and most noticeable symptoms that patients can monitor at home.
Night vision problems in diabetes occur when retinal photoreceptors become less sensitive in low-light conditions. Research shows diabetes slows dark adaptation and reduces night vision, even before visible diabetic retinopathy develops.
High glucose levels can impair rhodopsin regeneration and rod photoreceptor function. This reduces the eye’s ability to adjust to darkness, causing the need for brighter light and longer adaptation time.
Rod cells, responsible for night and peripheral vision, are particularly vulnerable in diabetes. Early rod dysfunction leads to difficulty driving at night, reading in dim light and navigating low-light environments.
These night-vision changes often appear early in diabetic eye disease, making prompt evaluation important for detecting retinal dysfunction.
Advanced peptide research using specific amino acid sequences shows promise for diabetic complications in many body systems. New delivery methods like glucose-responsive systems and pH-sensitive coatings improve how well peptides work.
MOTS-c shows strong benefits for diabetes management by improving insulin sensitivity and glucose metabolism. It also delays the onset of autoimmune diabetes by protecting pancreatic β-cells through targeted cellular pathways.
Researchers believe that bifunctional agonists such as tirzepatide will become more common in treating diabetes. Nanoparticle technology improves peptide stability and absorption. It also lowers how often doses are needed.
Results of these studies encourage research labs around the world to keep developing peptides. These target nerve protection, heart health, and blood sugar control at the same time.
These new therapies are potential clinical use cases that may change how we treat diabetes in the next ten years.
All products discussed are supplied for research purposes only and are not intended for human use.
(1) Brines M, Dunne AN, van Velzen M, Proto PL, et al. ARA 290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic symptoms in patients with type 2 diabetes. Mol Med. 2015 Mar 13;20(1):658-66.
(2) Wang RL, Yang ZH, Huang YY, Hu Y, et al. Erythropoietin-derived peptide ARA290 mediates brain tissue protection through the β-common receptor in mice with cerebral ischemic stroke. CNS Neurosci Ther. 2024 Mar;30(3):e14676.
(3) Al-Onaizi MA, Thériault P, Lecordier S, Prefontaine P, et al. Early monocyte modulation by the non-erythropoietic peptide ARA 290 decelerates AD-like pathology progression. Brain Behav Immun. 2022 Jan;99:363-382.
(4) Kong BS, Lee C, Cho YM. Mitochondrial-Encoded Peptide MOTS-c, Diabetes, and Aging-Related Diseases. Diabetes Metab J. 2023 May;47(3):315-324.
ALL CONTENT AND PRODUCT INFORMATION AVAILABLE ON THIS WEBSITE IS FOR EDUCATIONAL PURPOSES ONLY.
DISCLAIMER: These products are intended solely as a research chemical only. This classification allows for their use only for research development and laboratory studies. The information available on our Peptide Works website: https://peptide-works.com/ is provided for educational purposes only. These products are not for human or animal use or consumption in any manner. Handling of these products should be limited to suitably qualified professionals. They are not to be classified as a drug, food, cosmetic, or medicinal product and must not be mislabelled or used as such.
Peptide Works
Related Articles

Is Thymalin a Tissue Repair Peptide Therapy?
Have you ever wondered how the body begins to repair itself after injury or stress? Researchers are asking the same

Enhancing Energy with NAD+ Supplements
Energy is the driving force behind focus, movement, and recovery. When cells have less energy to work with, the body

The Role of L-Glutathione in Fighting Oxidative Stress
L-Glutathione plays a key role in controlling oxidative stress at the cellular level. It acts as a primary antioxidant that